

NATURAL HISTORY OF DISEASE
- 1. NATURAL HISTORY OF DISEASE Presenter Dr. Soumya Swaroop Sahoo JR, Dept. of Community Medicine
- 2. Contents • Introduction • Models of disease causation • Factors of disease causation • Natural history of disease in man • Levels of prevention • Quantifying prognosis
- 3. Definition • Natural history of disease refers to the progress of a disease process in an individual over time, in the absence of intervention. • The process begins with exposure to or accumulation of factors capable of causing disease. • Without medical intervention, the process ends with – recovery , – disability, – or death.
- 4. Exposure host disease recovery disability death Natural History of Disease
- 5. Natural History of Disease • Knowledge of the natural history of disease ranks alongside causal understanding in importance for disease prevention and control. • Natural history of disease is one of the major elements of descriptive epidemiology.
- 6. Natural History of Disease • The natural history of disease is best established by cohort studies. • As these studies are costly and laborious, understanding of the natural history of disease is largely based on other epidemiological studies, such as cross-sectional and retrospective studies, undertaken in different population settings.
- 7. Natural History of Disease • What the physician sees in the hospital is just an “episode” in the natural history of disease. • The epidemiologist, by studying the natural history of disease in the community setting is in a unique position to fill the gaps in the knowledge about the natural history of disease.
- 8. Natural History of Disease • The natural history and spectrum of disease presents challenges to the clinician and to the public health worker. • Because of the clinical spectrum, cases of illness diagnosed by clinicians in the community often represent only the “tip of the iceberg.” Many additional cases may be too early to diagnose or may remain asymptomatic. • For the public health worker, the challenge is that persons with undiagnosed infections may nevertheless be able to transmit them to others.
- 9. ICEBERG CONCEPT OF DISEASE DEATH SEVERE DISEASE MILD ILLNESS INFECTION WITHOUT CLINICAL ILLNESS EXPOSURE WITHOUT INFECTION CLINICAL DISEASE SUBCLINICAL DISEASE
- 10. Models of disease causation
- 11. Models of disease causation • Germ theory of disease • Epidemiological Triad • Epidemiological Tetrad • BEINGS theory • Web of Causation theory • Wheel theory
- 12. Germ Theory of Disease • Proposed by Robert Koch and Louis Pasteur. • Every human disease is caused by a microbe or germ, which is specific for that disease and one must be able to isolate the microbe from the diseased human being. ROBERT KOCH LOUIS PASTEUR
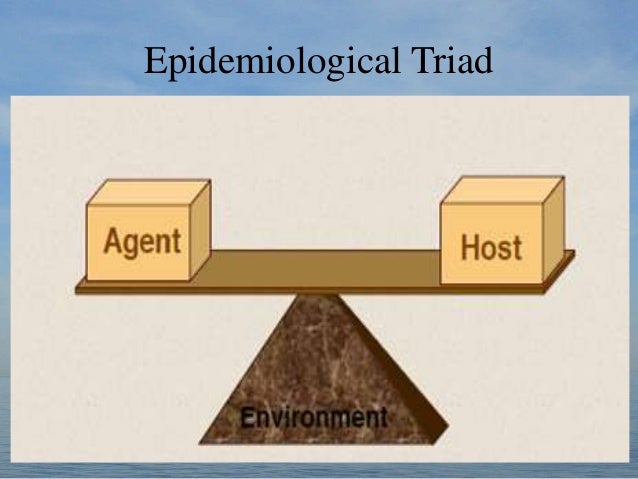
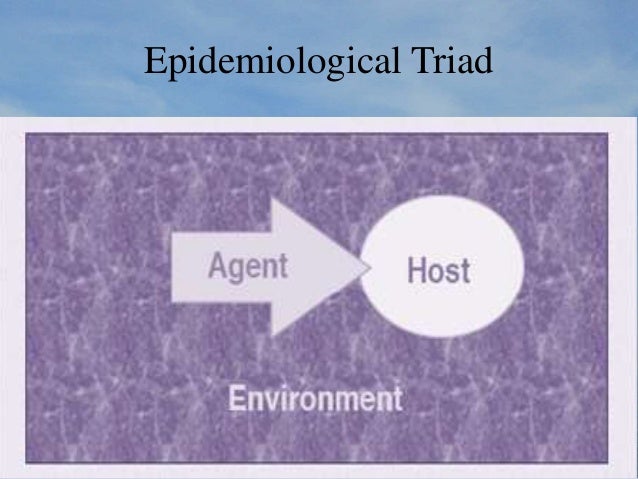
- 13. Epidemiological Triad
- 14. Epidemiological Triad
- 15. Agent • Is an element or substance, animate or inanimate, the presence (or absence) of which may initiate or perpetuate a disease process. • A disease may have a single agent, a number of independent alternative agents or complex of two or more factors whose combined presence is essential for the development of the disease.
- 16. Agent • Classification of agents: – Biological – Nutrient – Physical – Chemical – Mechanical – Absence or insufficiency or excess of a factor necessary to health – Social
- 17. Agent characteristics • Infectivity refers to the proportion of exposed persons who become infected. • Pathogenicity refers to the proportion of infected persons who develop clinical disease. • Virulence refers to the proportion of persons with clinical disease who become severely ill or die.
- 18. Agent characteristics • Hepatitis A virus in children has low pathogenicity and low virulence, since many infected children remain asymptomatic and few develop severe illness. • In persons with good nutrition and health, measles virus has high pathogenicity but low virulence, since almost all infected persons develop the characteristic rash and illness but few develop the life- threatening presentations of measles (pneumonia, encephalitis). • In persons with poor nutrition and health, measles is a more virulent disease, with mortality as high as 5-10%. • Rabies virus is both highly pathogenic and virulent, since virtually 100% of all infected persons (who do not receive treatment) progress to clinical disease and death.
- 19. Host • In epidemiological terminology, the human host is referred to as “soil” and the disease agent as “seed”. • A person or other living animal, that affords subsistence or lodgment to an infectious agent under natural condition. • Host factors: Intrinsic factors that influence an individual’s exposure, susceptibility, or response to a causative agent.
- 20. Environment • Physical environment – Non living things and physical factors(air, water, soil, housing, heat, light, etc) • Biological environment – Microbial agents, insects, animals, plants and man himself. • Psychosocial environment – Lifestyle, poverty, urbanization, community life, income, education, stress etc.
- 21. AGENT HOST FACTORS ENVIRONMENT FACTORS 1.Poor housing 2.Overcrowding 3.Poverty 4.Urbanization 1.Decreased immunity 2.Malnutrition 3.Elderly 4.HIV infectionM. Tuberculosis
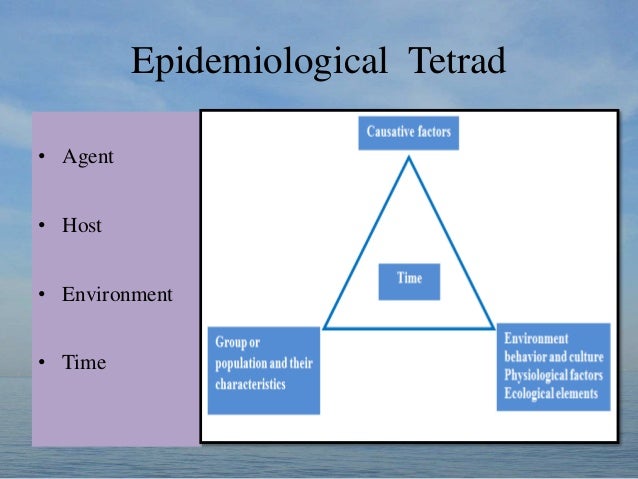
- 22. Epidemiological Tetrad • Agent • Host • Environment • Time
- 23. Disease Occurrence • Different diseases, in different communities, show different patterns of expected occurrence: • Endemic: habitual presence of a disease within a given geographic area. • Hyperendemic :a persistently high level of occurrence. • Sporadic : an irregular pattern of occurrence, with occasional cases occurring at irregular intervals.(prevalence is zero)
- 24. Disease Occurrence • Epidemic: occurrence in a community or region of a group of illnesses of similar nature, clearly in excess of normal expectancy and derived from a common or from a propagated source. • Public health officials often use the term outbreak, which means the same, because it is less provocative to the public. • When an epidemic spreads over several countries or continents, affecting a large number of people, it is called a pandemic(worldwide epidemic).
- 25. The “BEINGS” Model of Disease Causation • This concept postulates that human disease and its consequences are caused by a complex interplay of nine different factors – – Biological factors innate in a human being, – Behavioural factors concerned with individual lifestyles, – Environmental factors as physical, chemical and biological aspects of environment, – Immunological factors, – Nutritional factors, – Genetic factors, – Social factors, – Spiritual factors and – Services factors, related to the various aspects of health care services.
- 26. The Theory of “Web of Causation” • The “epidemiological triad theory” was very effectively used by Leavel and Clark in explaining the natural history of disease and levels of prevention for obviating such departures from the state of health. • But it could not explain the causation of non communicable diseases like IHD or road accidents.
- 27. Web of causation • McMahon and Pugh forwarded the theory of “epidemiological web of causation”, wherein the various factors (e.g. hypercholesterolemia, smoking, hypertension) are like an interacting web of a spider. • Each factor has its own relative importance in causing the final departure from the state of health, as well as interacts with others, modifying the effect of each other.
- 28. Web of Causation applied to Myocardial Infarction
- 29. Example of Web of Causation Susceptible Host Infection Tuberculosis Vaccination Genetic Overcrowding Malnutrition Tissue Invasion and Reaction Exposure to Mycobacterium
- 30. Application of the Web Epidemiologic Triad • devised to enhance search for understanding communicable disease Web of Causation • devised to address non-communicable diseases – can also be applied to communicable disease
- 31. Wheel theory • As medical knowledge advanced, an additional aspect of interest that came into play is the comparative role of “genetic” and the “environmental” (i.e. extrinsic factors outside the host) factors in causation of disease. • The “triad” as well as the “web” theory does not adequately cover up this differential. • To explain such relative contribution of genetic and environmental factors, the “wheel” theory has been postulated.
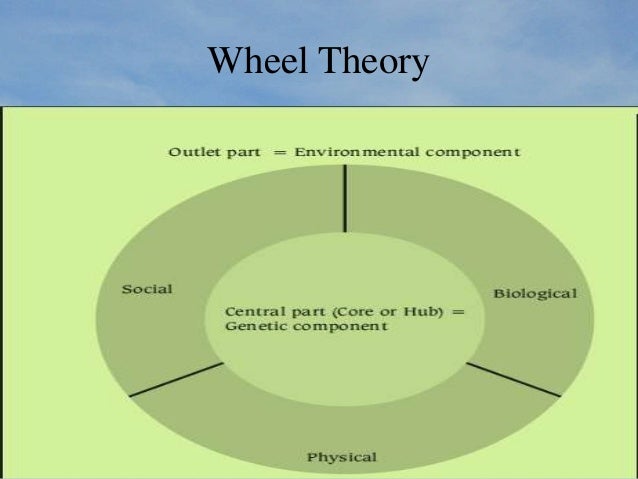
- 32. Wheel theory • The theory visualizes human disease in the form of a wheel, which has a central hub representing the genetic components and the peripheral portion representing the environmental component. • Like any wheel, the outer part (environmental component) has spokes (3 in this model) and the environmental component is thus divided into 3 sub components, representing the social, biological and physical components of the environment.
- 33. Wheel Theory
- 34. Wheel Theory
- 35. Factors of disease causation
- 36. Factors of Disease Causation • a) Predisposing factors are factors which create a state of susceptibility, so that the host becomes vulnerable to the agent or to necessary cause, e.g. age, sex, previous illness. • b) Enabling factors are those which assist in the development of (or in recovery from) the disease; e.g. housing conditions, socio-economic status. • c) Precipitating factors are those which are associated with immediate exposure to the disease agent or onset of disease, e.g. drinking contaminated water, close contact with a case of pulmonary TB.
- 37. Factors of Disease Causation • d) Reinforcing factors are those which aggravate an already existing disease, e.g. malnutrition, repeated exposures • e) Risk factors : A risk factor is defined as a condition, quality or attribute, the presence of which increases the chances of an individual to have, develop or be adversely affected by a disease process. A risk factor is not necessarily the cause of a disease but does increase the probability that a person exposed to the factor may get the disease.
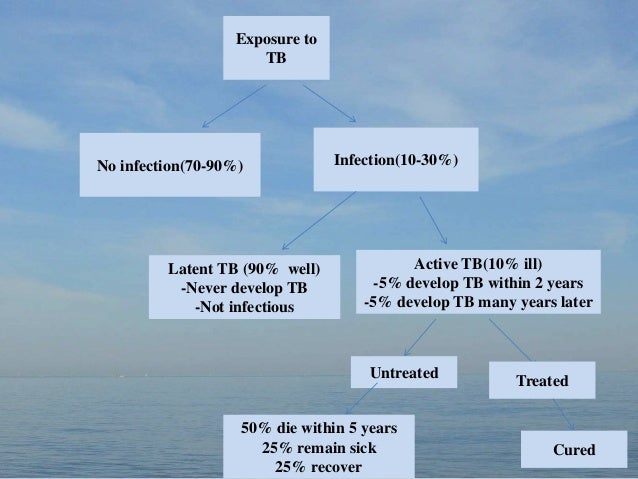
- 38. Exposure to TB Infection(10-30%)No infection(70-90%) Active TB(10% ill) -5% develop TB within 2 years -5% develop TB many years later Latent TB (90% well) -Never develop TB -Not infectious Treated Untreated Cured 50% die within 5 years 25% remain sick 25% recover
- 39. The Natural history of disease in man
- 40. (A) (P) (S) (M) (D) (T) The Natural history of disease in a patient • A ; Biologic onset of disease • P ; Pathologic evidence of disease if Sought • S ; Signs and symptoms of disease • M ; Medical care sought • D ; Diagnosis • T ; Treatment Preclinical Phase Clinical Phase Gordis L. Epidemiology. WB Saunders Company. 1996
- 41. Primordial prevention • Prevention of the emergence or development of risk factors. • Particularly useful for chronic diseases. • Example :Many adult health problems (e.g., obesity, hypertension) have their early origins in childhood, because this is the time when lifestyles are formed (smoking, eating patterns, physical exercise). • Efforts are directed towards discouraging children from adopting harmful lifestyles . • The main intervention – is through individual and mass education.
- 42. Primary prevention • Measures of prevention undertaken during the phase of pre- pathogenesis (phase of susceptibility) • Involves two sub-steps: Health promotion and specific protection • Health Promotion : Steps undertaken to improve the level of general health and well being so that conditions for initiation of disease process are prevented. • These steps are not specific for any disease or a group of diseases.
- 43. Primary prevention • It includes – improvement in the overall socio-economic status of the population, – health education, – feeding programmes for mothers and children, – promotion of breast feeding, – promotion of small family norms, – education – motivation for healthy lifestyle.
- 44. Primary prevention • Specific Protection : include measures to prevent the initiation of specific diseases or a group of diseases. • Examples – Immunization to protect against specific diseases – Fortification of foods with specific nutrients (as salt with iodine) – Use of condoms to protect against sexually transmitted diseases (STDs) – Use of helmets to protect against head injuries
- 45. Primary prevention • Both health promotion and specific protection are type of “primary preventive” strategy. • However, health promotional approach improves the general health so that a number of diseases are aimed at. • For example, by promoting breast feeding among children, we try to prevent general malnutrition, vitamin A deficiency, providing antibodies against various diseases, preventing diarrhoeal diseases. • On the other hand when condom is used, it is for a very specific group of diseases i.e. STDs; when measles vaccine is given it is for a specific disease viz. measles.
- 46. Primary prevention • Two types of strategy: – Population strategy – High risk strategy
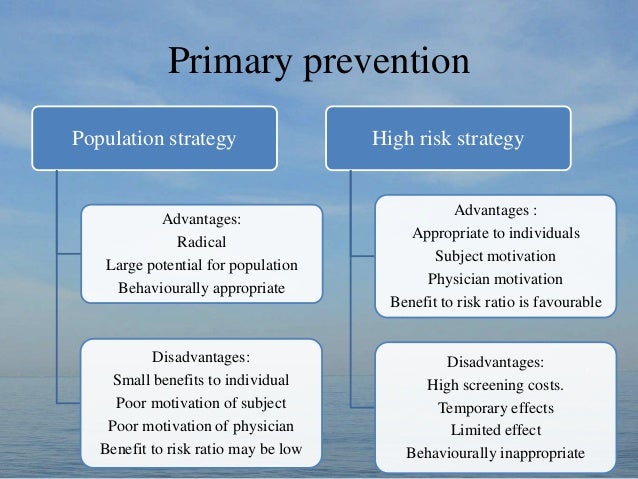
- 47. Primary prevention Population strategy Advantages: Radical Large potential for population Behaviourally appropriate Disadvantages: Small benefits to individual Poor motivation of subject Poor motivation of physician Benefit to risk ratio may be low High risk strategy Advantages : Appropriate to individuals Subject motivation Physician motivation Benefit to risk ratio is favourable Disadvantages: High screening costs. Temporary effects Limited effect Behaviourally inappropriate
- 48. Prevention Paradox • A preventive measure which brings much benefit to the population often offers little to each participating individual. • Classical example is the Framingham study: – Data from the study suggests that if all men upto age 55 reduced their cholesterol level by 10%, 1 in 50 could expect to avoid a heart attack on average, yet 49 out of 50 would follow the same measures and perhaps get nothing out of it.
- 49. Secondary Prevention • These include all actions undertaken at the stage of early pathogenesis (asymptomatic disease) with a view to halt the progress of disease at it’s earliest, incipient stage, by “early diagnosis and prompt treatment”. – classical example is “screening for disease” for breast cancer (using mammography) and cervical cancer (using pap smear). – medical examinations of school children, of industrial workers and various disease screening camps.
- 50. Tertiary prevention • These include all measures undertaken when the disease has become clinically manifest or advanced, with a view to prevent or delay death, reduce or limit the impairments and disabilities, minimize suffering and to promote the subject’s adjustment to irremediable conditions. • Tertiary prevention has two types of approaches : – disability limitation – rehabilitation.
- 51. Tertiary prevention • Disability Limitation : These include all measures to prevent the occurrence of further complications, impairments, disabilities and handicaps or even death. example : – Application of plaster cast to a patient who has suffered Colle’s fracture, is done to prevent complications and further disability like mal-union or non-union. – Complete rest, morphine, oxygen and streptokinase is given to a patient of Acute MI, to prevent death or complications like arrhythmias / CHF.
- 52. Tertiary prevention • The sequence with which a disease turns into a handicap is as follows : – Disease : This is a pathological process and it’s manifestations which indicate a departure from the state of perfect health. – Impairment : This is the actual loss or damage of a part of body anatomy or an aberration of the physiological functions that occurs consequent to a disease. – Disability : This is defined as the inability to carry out certain functions or activities which are otherwise expected for that age / sex, as a result of the impairment. – Handicap : This is the final disadvantage in life which occurs consequent to an impairment or disability, which limits the fulfillment of the role a person is required to play in life.
- 53. Tertiary prevention • Rehabilitation : This is the second component of tertiary prevention. • Rehabilitation stands for the combined and coordinated usage of all the available medical, social, educational and vocational measures, for training the person to the highest level of functional ability.
- 54. Tertiary prevention • Medical rehabilitation : – This is done through medical / surgical procedures to restore the anatomy, anatomical functions and physiological functions to as near normal as possible. • Vocational rehabilitation : – It includes steps involving training and education so as to enable the person to earn a livelihood. • Social rehabilitation : – This involves steps for restoration of the family and social relationships. • Emotional and Psychological rehabilitation : – This involves steps to restore the confidence, personal dignity and confidence.
- 55. Levels of Prevention Level of prevention Phase of disease Target Primordial Underlying condition leading to causation Total population and selected groups Primary Specific causal factors Total population, selected groups and healthy individuals Secondary Early stage of disease Patients Tertiary Late stage of disease Patients
- 56. Quantifying the Prognosis • Prognosis is a quantitative expression of the likelihood of a specific outcome (survival). Prognosis Death CFR Survival 5 year survival Observed survival Median survival Relative survival
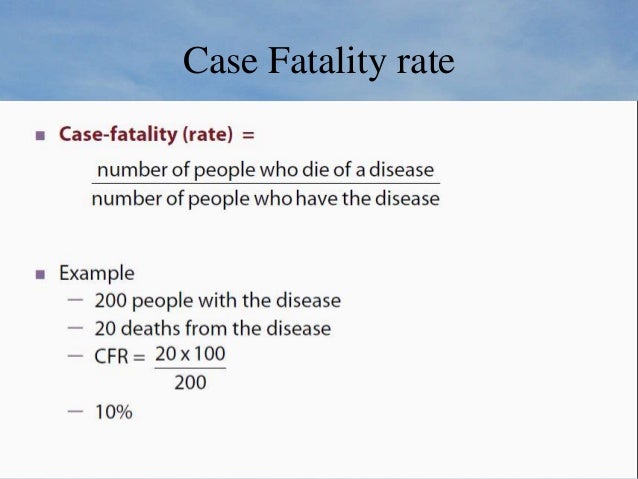
- 57. Case Fatality rate
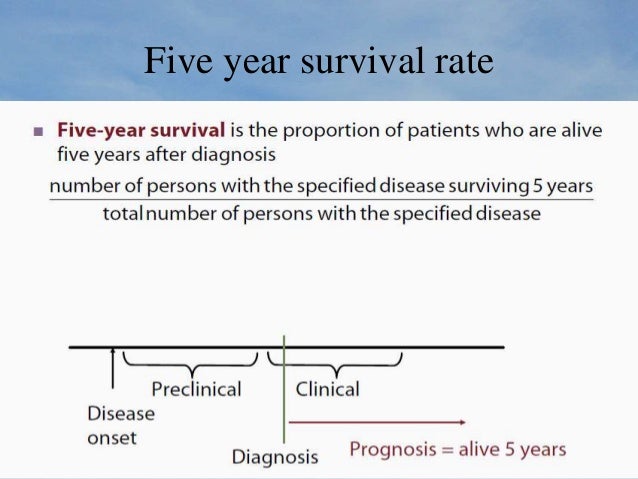
- 58. Five year survival rate
- 59. Five year survival rate • Widely used in cancer studies • Eg. The five-year survival rate for women with – Localized (stage I) breast cancer: 88% – Metastatic Stage 4 breast cancer:15%
- 60. Lead Time • Lead time is the time between the early detection of disease (e.g by screening) and the time of its usual clinical diagnosis. • Lead time bias occurs because of the failure to account for the lead time when calculating survival.
- 61. Observed survival rate • The observed survival rate is an estimate of the probability of surviving. • Probability of surviving can be calculated using the technique of life table analysis. • Advantage of using data on all patients, regardless of how long they survive.
- 62. Median survival time • Median survival time is the length of time that half of the study population survives. • Advantages over mean survival: – Less affected by extremes. – Have to study only half the group.
- 63. Relative survival rate • Relative survival rate is the ratio of the observed survival (rate) to the expected survival (rate) • It compares survival in the study group (e.g., cancer) to the survival of a comparable group without the disease of interest. • It removes from the observed survival the effect of deaths from all other causes. • Comparison group consists of persons in the general population similar to the patient group with respect to age, sex, and calendar year of observation, and free of the disease of interest.
- 64. References • Park’s Textbook of preventive and social medicine, 21st edition • Textbook of Epidemiology, Leon Gordis, 4th edition. • Textbook of public health and community medicine, AFMC,2009 • Measures of prognosis, Bloomberg School of Public Health,2008 • CDC , Principles of Epidemiology in Public Health Practice, 3rd Edition










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}